Metastatic Prostate Cancer
A 47 years old Caucasian male with a history of metastatic prostate adenocarcinoma (diagnosed 2 years ago when he presented with obstructive uropathy and elevated PSA, had retroperitoneal lymphadenopathy and Gleason score of 5+5=10, highest grade, was treated with chemotherapy and androgen blockade with good response) presented with rising PSA (increase from 0.1 to 10.1 ng/ml), despite radiographic improvement in the prostate on recent CT and a negative whole body bone scan.
Currently, no urinary or GI complaints.
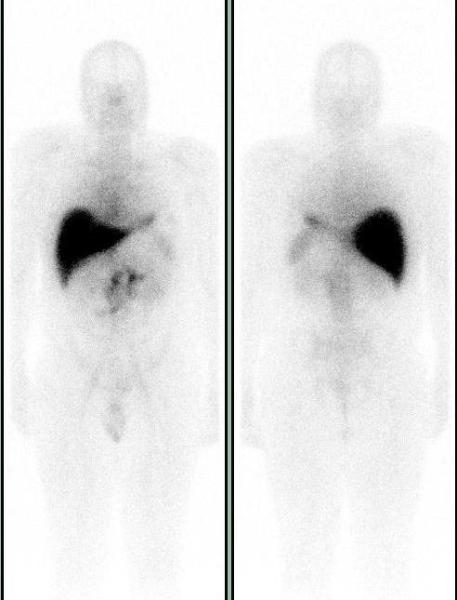
A Prostascint study was ordered to determine the cause of the rising PSA. Five days after the injection of 7.0 mCi of In-111 Capromab pendetide (prostascint – Indium labeled monoclonal antibody that reacts with (PSMA) prostate specific membrane antigen) whole body images were acquired in anterior and posterior projections and SPECT-CT images of the abdomen and pelvis were acquired. Unlike PSA, PSMA is a membrane glycoprotein that correlates with the aggressiveness of malignancy. It is expressed in all prostate tissue, malignant and benign. The conjugated antibody also binds duodenal epithelial cells and proximal tubule cells in the kidney.
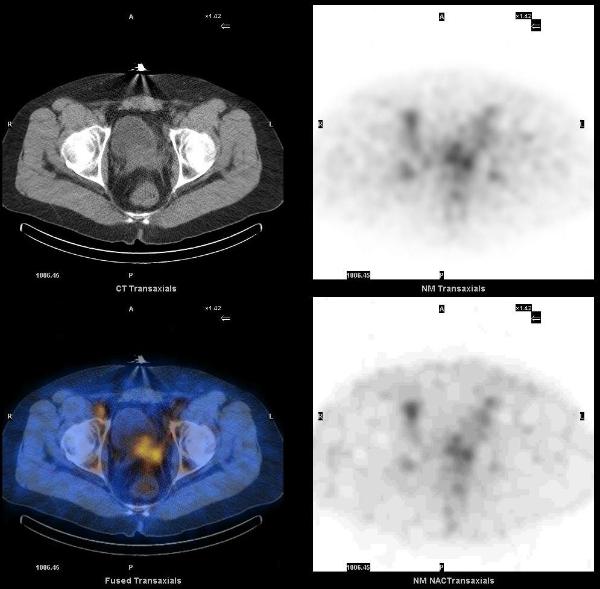
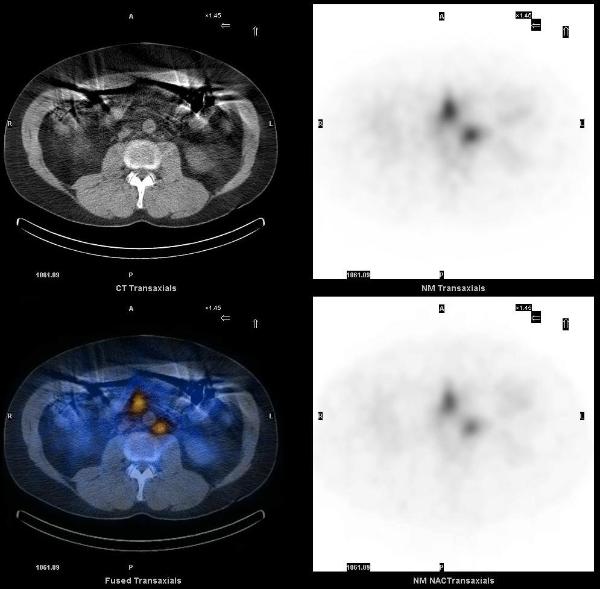
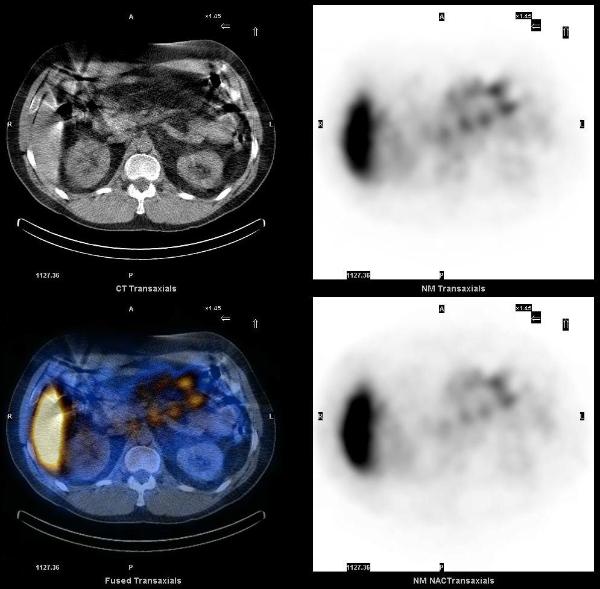
On SPECT-CT images, ProstaScint uptake is noted in prostate gland and in several retroperitoneal lymph nodes, particularly in the left para-aortic region. There are also foci of increased uptake in the central abdomen and left upper quadrant, which correspond to mesenteric lymph nodes.
1. Manyak MJ. Indium-111 capromab pendetide in the management of recurrent prostate cancer. Expert Rev Anticancer Ther. 2008 Feb;8(2):175-81.
2. Chang, SS. Overview of Prostate-Specific Membrane Antigen. Rev Urol. 2004; 6 (Suppl 10): S13–S18.
This case was compiled by Dr. Vivek Bansal, BCM